
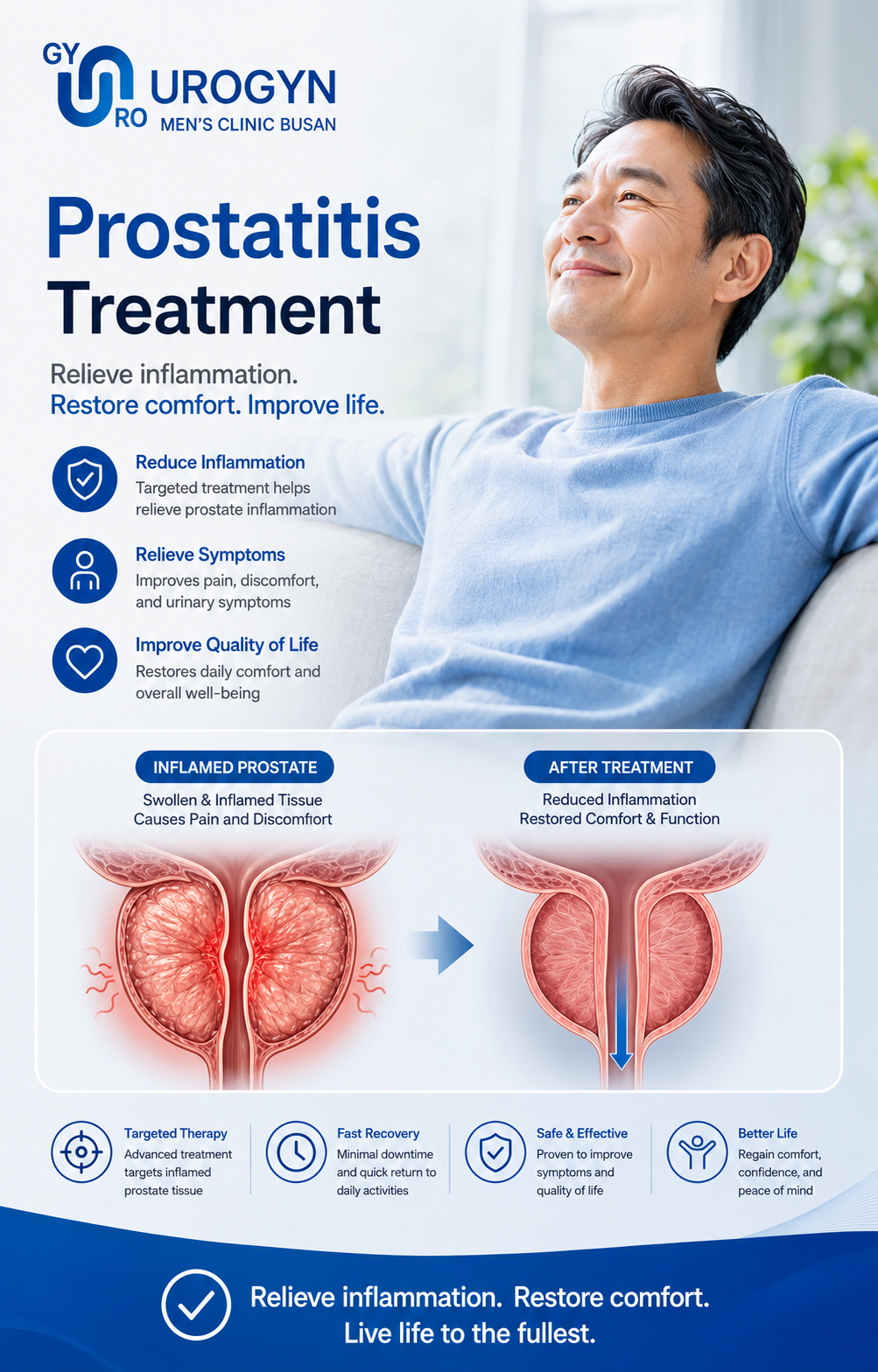
Prostatitis treatment — a real diagnosis, not another antibiotic.
Most men with chronic prostatitis have been handed repeat antibiotic courses that never fixed the problem — because the type was never properly identified. We start by finding out which of the four kinds of prostatitis you actually have, then build a targeted program: culture-directed antibiotics, alpha-blockers, pelvic-floor therapy or low-intensity shockwave, in English, with one urologist managing your case.
“Most men sent to us have taken antibiotics three or four times for prostatitis that was never bacterial in the first place. The fix isn't a stronger antibiotic — it's the right diagnosis. Once we know which type you have, the treatment usually becomes straightforward.”
— Dr. Moon Hyeon-chang, Director
Prostatitis, by the numbers.
Understanding the condition is half the battle — and it's why the wrong treatment is so common.
The four types of prostatitis.
They look similar but are treated completely differently. Getting this right is the whole game — and exactly what repeat antibiotics skip.
Acute bacterial
Sudden fever, chills, painful urination and a tender prostate. A genuine infection that needs prompt, culture-directed antibiotics.
Chronic bacterial
Recurrent urinary infections with the same organism returning after antibiotics stop. Needs a longer, properly targeted antibiotic course.
CPPS (non-bacterial)
Pelvic, perineal or testicular pain for 3+ months with no bacteria found. Antibiotics won't help — this needs multimodal therapy.
Asymptomatic
Inflammation found incidentally during a fertility or PSA work-up, with no symptoms. Often needs no treatment beyond monitoring.
Symptoms men come to us with.
Any combination lasting more than a few weeks is worth a proper evaluation — especially if antibiotics haven't helped.
Why antibiotics keep failing you.
If round after round hasn't worked, it's almost never the drug — it's the diagnosis underneath it.
It was never bacterial
Around 90% of chronic prostatitis is CPPS, with no infection to kill. Antibiotics can't fix a problem that isn't an infection — so the symptoms simply return.
No culture was taken
Even when it is bacterial, treating without a culture means guessing the organism and the course length. We localize and target it properly before prescribing.
The pelvic floor was ignored
Much chronic pelvic pain is driven by tight pelvic-floor muscles and nerve sensitization. No pill addresses that — physical therapy and shockwave do.
The work-up that ends the guessing.
One focused visit to classify your prostatitis correctly — so the treatment that follows is the right one.
NIH-CPSI symptom score
A validated questionnaire that quantifies pain, urinary symptoms and quality-of-life — and lets us track your progress objectively over time.
Urinalysis & culture
Identifies infection and the exact organism, so any antibiotic is targeted rather than guessed.
Localization test (EPS / 2-glass)
Expressed prostatic secretion or pre/post-massage urine pinpoints whether bacteria are coming from the prostate itself — the step that separates Type II from CPPS.
Uroflowmetry + PSA
Flow study to rule out obstruction, plus PSA screening — important because BPH and, rarely, cancer can mimic prostatitis.
Matched to your type , not a one-size script.
Bacterial types get targeted antibiotics. CPPS gets a combined program — usually two or three of these together, adjusted as you respond.
Culture-directed antibiotics
For Type I & II only. The right drug for the cultured organism, for the right length (often 4–6 weeks in chronic bacterial cases) — not a blind repeat course.
Alpha-blockers
Relax the bladder neck and prostate to ease flow, urgency and pressure — useful in both bacterial and CPPS cases.
Anti-inflammatory & phytotherapy
Targeted anti-inflammatories and evidence-supported plant extracts to calm prostatic and pelvic inflammation in CPPS.
Pelvic-floor physical therapy
The core of modern CPPS care: releasing tight, over-active pelvic-floor muscles and retraining them — addressing the driver pills can't reach.
Low-intensity shockwave (LiESWT)
Focused acoustic-wave therapy that reduces chronic pelvic pain and improves blood flow — a growing, well-tolerated option for stubborn CPPS.
Triggers & lifestyle
Identifying and removing flare triggers — caffeine, alcohol, prolonged sitting, stress — so gains from treatment actually hold.
How fast you'll feel better.
It depends entirely on type — so we're clear with you from day one.
Bacterial (Type I / II)
- Acute infections often improve within days of the right antibiotic
- Chronic bacterial needs a longer 4–6 week targeted course
- Cure is realistic once the organism is correctly identified
- We confirm clearance rather than just stopping the drug
CPPS (Type III)
- Managed, not "cured overnight" — think weeks, not days
- Most men see meaningful relief over 6–12 weeks of combined therapy
- Pelvic-floor therapy and shockwave build over a course of sessions
- We adjust the program by your NIH-CPSI score as you go
Worried it might be flow, not pain? Compare with our prostate care overview and BPH options like UroLift or Rezum.
Begin with a proper evaluation.
One focused visit to classify your prostatitis — then a treatment program and transparent quote built around what we find.
Prostatitis evaluation
Because prostatitis treatment varies so much by type, we price the evaluation up front and quote the program transparently once we know the cause — no open-ended bills. Itemized English receipts on request.
From first visit to steady relief.
Diagnose & start
Symptom scoring, cultures and a localization test classify your type the same day. Treatment begins immediately — antibiotics if bacterial, or the first CPPS measures.
Early response
Bacterial cases usually start easing quickly. For CPPS, alpha-blockers and anti-inflammatories take the edge off while pelvic-floor work begins.
Build the program
Chronic bacterial courses complete with confirmed clearance. CPPS therapy — pelvic-floor sessions and, if needed, shockwave — builds toward meaningful relief.
Review & adjust
We re-score your NIH-CPSI remotely, confirm what's working and fine-tune. Most CPPS patients are clearly better by this point and managing flares confidently.
Tell us what you're feeling — before you fly.
A free video consultation. Describe your symptoms and history, send any prior test results, and get an honest read on what's likely going on. No commitment.
Replies within 24 hours · KST 9am–9pm
Your visit, step by step.
From the first WhatsApp message to flying home — here's the path most international patients follow.

Free video consult
Send your symptoms and history over WhatsApp. The doctor reviews your case in English and explains likely options and cost.

Diagnosis & testing
On-site tests confirm your condition and rule out other causes — so the plan fits your anatomy before anything is decided.

Begin treatment
Your treatment program is set by a board-certified urologist — antibiotics, alpha-blockers, pelvic-floor therapy or shockwave — started while you are here.

Recovery & aftercare
Fly home when cleared. Your doctor stays reachable on WhatsApp for 6 months of follow-up — photos, questions, guidance.
Your medical team.
Board-certified urologists — the doctor who consults with you is the same one who performs your procedure and follow-up.

Dr. Moon Hyeon-chang
- Board-certified urologist, 15+ years
- AUA · EAU · WAS · KSSM member
- Direct English consultation
- Patients from 40+ countries
Dr. Kim Tae-kyung
- Board-certified urologist
- BPH focus — UroLift & Rezum
- MD & MS, Pusan National University
- Adjunct Prof, Ulsan Univ Hospital

Dr. Kim Jin-seong
- Board-certified, Gyeongsang Nat'l Univ
- Korean Prostate Society member
- Adjunct Clinical Prof, GNU Hospital
- Men's health & prostate surgery
Before you reach out.
Most likely because it was never bacterial. Around 90% of chronic prostatitis is CPPS — chronic pelvic pain with no infection — and antibiotics can't fix a problem that isn't an infection. The first thing we do is test which type you actually have, so you stop taking drugs that were never going to work.
With a localization test — expressed prostatic secretion or a pre/post-massage (2-glass) urine test — alongside a urine culture. These show whether bacteria are actually coming from the prostate. If cultures are negative and pain has lasted three months or more, it's CPPS, which is treated very differently from a true infection.
CPPS is managed rather than "cured" with a single pill, but most men achieve real, lasting relief with a combined program — alpha-blockers, anti-inflammatories, pelvic-floor physical therapy and, for stubborn cases, low-intensity shockwave. Improvement typically builds over 6–12 weeks, and we track it objectively with your NIH-CPSI score.
Usually not. Most prostatitis — especially CPPS — is not an STI and isn't contagious. Some acute bacterial cases can involve organisms linked to STIs, which is exactly why we culture and identify the organism rather than assume. Your evaluation clarifies this directly.
It can. Chronic pelvic pain and inflammation may contribute to painful ejaculation, reduced desire or erectile difficulty, and some types can affect semen quality. Treating the underlying prostatitis often improves these — and if needed, we can address sexual or fertility concerns alongside it.
If you've already had repeat antibiotics that failed, the value is in the diagnosis you haven't had yet — proper localization testing, type classification and a multimodal CPPS program in English, all in one focused visit. Many international patients come specifically because that full work-up and pelvic-floor/shockwave option wasn't offered at home.
A focused visit: consultation and history, NIH-CPSI scoring, urinalysis and culture, a localization test, uroflowmetry and PSA — ending in a clear type diagnosis and a written plan. Because treatment varies so much by type, we quote the evaluation up front and price the program transparently once we know the cause, with itemized English receipts on request.
Yes. The board-certified urologist who consults with you is the same doctor who diagnoses your prostatitis and manages your follow-up — one specialist from start to finish. You are never passed to a junior doctor or a different physician.
Explore the other options.
Tap to jump to another prostate-care page.